Why the Correct Code Depends on Contrast, Not on What Was Ordered
CPT code 71250 billing content across the field treats consulting a Clinical Decision Support Mechanism as a live compliance requirement with real payment consequences. It isn’t.
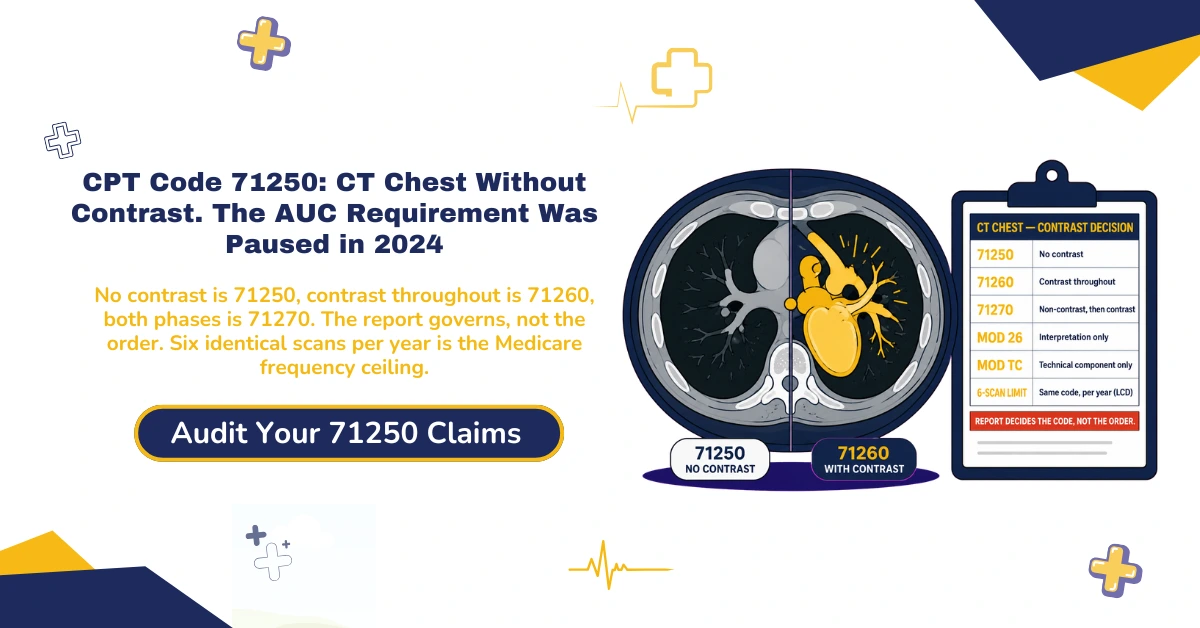
CMS paused the entire Appropriate Use Criteria program and rescinded its own implementing regulation, 42 CFR 414.94, effective January 1, 2024. No resumption date has been announced since.
No claim has ever been denied, and no payment penalty has ever applied, for skipping that consultation at any point since the program began.
A practice still building CDSM checks into its imaging workflow is maintaining infrastructure against a rule that currently carries no payment consequence at all.
The correct CPT code for a chest CT depends on one variable: whether contrast material was administered, not administered, or administered after an initial non-contrast phase.
Three codes cover this single anatomic region on that basis alone. 71250 runs without contrast, 71260 with contrast, and 71270 without contrast followed by with contrast.
The report decides which of the three applies. That single fact prevents the most common coding error on this study, and the rest of this guide builds on it.
Anyone billing CPT code 71250 in 2026 needs the current answer, not the one the field keeps repeating from the program’s testing years.
This reference covers the correct modifier for every billing arrangement, the exact frequency limit Medicare applies to repeat scans, and the complete, accurate AUC and CDSM history.
It also covers the shared medical necessity list behind all three contrast-status codes, the line between routine diagnostic CT and low-dose lung cancer screening, and the prior authorization a Radiology Benefit Manager enforces today.
What CPT Code 71250 Actually Covers
CPT 71250 covers a computed tomography examination of the thorax performed without contrast material, a single cross-sectional acquisition of the lungs, mediastinum, pleura, and chest wall.
That’s the anatomic scope for all three contrast-status codes. What separates 71250 from the other two is the absence of contrast, nothing else about the anatomy or the acquisition.
The AMA Descriptor and What It Includes
The base study includes thin-section axial images with standard reconstructions, and multiplanar reformats where clinically indicated. Those reformats are inherent to the base service, not separately reportable.
High-resolution protocols used to evaluate interstitial lung disease don’t carry a separate CPT code. The base thorax code applies regardless of resolution protocol, with contrast status alone deciding which of the three codes fits.
Contrast, when it’s used, is captured by the contrast-status code itself, not billed as a separate line on top of 71250. The code already reflects whether contrast was part of the study.
Picture a chest CT ordered to characterize a lung nodule. The scanner captures one complete image set, the radiologist reads it, and absent contrast, 71250 is the correct base code.
Why the Professional and Technical Components Split
71250 carries a PC/TC indicator of 1. The professional and technical components can be billed separately, depending on who performs each part of the service.
The technical component covers the equipment, the technologist’s time, and the facility overhead needed to acquire the images. The professional component covers the radiologist’s interpretation and the written report.
That indicator is why the same code can generate two separate claims from two separate entities. Section 4 covers the modifiers that tell the payer which component each claim represents.
71250 vs 71260 vs 71270: The Contrast Decision, and Why the Report Governs, Not the Order
71250 applies when no contrast is administered. 71260 applies when contrast is administered throughout. 71270 applies when an initial non-contrast phase is followed by a contrast-enhanced phase in the same session.
71270 reimburses the highest of the three. It requires the radiologist to interpret two complete image sets, a non-contrast phase and a contrast-enhanced phase, from a single session.
The Three Codes, Compared
Read the three side by side and the pattern is plain: the more image sets the radiologist interprets, the higher the reimbursement.
| Code | Contrast status | What it covers and how it pays |
|---|---|---|
| 71250 | No contrast | Single non-contrast acquisition of the thorax. The base of the three rates. |
| 71260 | Contrast throughout | Single contrast-enhanced acquisition. Priced above 71250. |
| 71270 | Non-contrast, then contrast | Two complete image sets in one session. The highest of the three rates. |
The difference between 71250 and 71260 is contrast alone. The difference between either single-phase code and 71270 is a second, separately interpreted image set.
Contrast changes the study because it highlights vasculature and vascular lesions a non-contrast scan can’t resolve. That added interpretation, not a different anatomic region, is what separates 71260 from 71250.
The Documentation Rule That Prevents the Single Most Common Coding Error
The radiology report governs which code is correct, not what the order specified. If the order calls for a non-contrast study but the report documents contrast administration, CPT code 71250 is no longer correct, regardless of what was requested.
The report has to state explicitly whether contrast was used before a coder finalizes the claim. A coder working from the order alone will bill the wrong code the moment the two disagree.
71250 shouldn’t be billed alongside 71260 or 71270 for the same imaging session on the same date. Those codes are mutually exclusive for one study.
A narrow, well-documented exception exists for two truly distinct, separately medically necessary studies performed at different times on the same date. Each needs its own clear indication and Modifier 59, or the more specific XS, covered fully in Section 5.
Modifiers 26 and TC: Getting the Professional and Technical Split Right
Modifier 26 identifies the professional component: the radiologist’s interpretation and written report. Modifier TC identifies the technical component: the equipment, technologist, and facility work required to acquire the images.
A currently published competitor guide states this backwards, calling Modifier TC the professional component modifier. It isn’t. Reversing the two is a fast way to misroute a claim and trigger a mismatch denial.
Modifier 26, the Professional Component
Append Modifier 26 when the interpreting radiologist doesn’t own or operate the imaging equipment. That’s the typical setup for a facility-employed or contracted radiologist reading a study performed at a hospital, an imaging center, or through a teleradiology arrangement.
The modifier answers a single question for the payer: which slice of the service is this claim for? Get the answer wrong and the payment math stops adding up.
Modifier TC, the Technical Component
Append Modifier TC when the facility owns the scanner and employs the technologist, and it bills separately from the interpreting physician. TC captures the acquisition, not the read.
Global Billing, and the Duplicate-Payment Risk That Comes With Getting It Wrong
When one entity performs and interprets the study, bill the code globally, with no modifier at all. The global payment already equals both components combined.
Billing the global code and a component modifier together for the same study, or having both the facility and the physician bill globally, creates a duplicate payment that gets caught and recouped.
That duplicate carries real overpayment liability under the False Claims Act, not just a denial risk. The safer habit is to confirm who did what before choosing global or a component split.
Say an independent imaging center owns the scanner and employs the radiologist. One entity, one global claim, no modifier. Split that same study between a hospital and an outside reading group, and each bills its own component.
Modifier 59, XS, and When Two Chest CT Claims on One Date Are Legitimate
Two truly distinct, separately medically necessary chest CT studies performed at different times on the same date can both be billed.
The documentation has to support two independent reasons for imaging. Modifier 59, or the more specific XS where a payer recognizes it, distinguishes the second line from the first.
The Exception to Mutual Exclusivity
Before defaulting to Modifier 59 to unbundle two same-day chest CT claims, confirm first whether the combined without-and-with-contrast code, 71270, actually describes what was performed as a single continuous study.
Modifier 59 exists for genuinely distinct encounters, not as a workaround for a study that should have been billed as one combined code from the start. Reach for it only after 71270 is ruled out.
The order of operations matters. Rule out the single combined code, confirm two independent indications, document each separately, then apply the distinguishing modifier. Skipping the first step is the most common way this gets billed wrong.
A patient scanned once in the morning for one documented indication, then again that evening for a genuinely separate one, produces two legitimate lines, distinguished with XS where the payer recognizes it.
NCCI and the CT-Guided Biopsy Interaction
When a chest CT is integral to a same-day CT-guided biopsy or interventional procedure, the imaging component may already be included in the guidance code itself.
Verify current NCCI edits before separately reporting 71250 alongside an interventional radiology code performed the same date. Billing both without checking is how a bundled service turns into a recoupment.
The same caution applies when 71250 appears alongside other same-day imaging like a chest X-ray, 71046. Confirm the services are genuinely separate before billing both.
The AUC and CDSM Requirement, Stated Completely and Accurately
The Protecting Access to Medicare Act of 2014, Section 218(b), created a program requiring the ordering professional to consult a qualified Clinical Decision Support Mechanism before ordering advanced diagnostic imaging. CT was among the covered modalities for Medicare Part B beneficiaries.
What PAMA Actually Established in 2014
The mechanism was an electronic portal. The ordering provider would access appropriate use criteria before placing the order, and the furnishing facility would report which CDSM was consulted on the claim itself.
The Educational Testing Period That Never Carried a Penalty
Starting January 2020, CMS directed ordering providers to begin this consultation in an educational and operations testing period.
During that entire period, no claim was ever denied and no payment penalty was ever applied for failing to consult a CDSM. The testing phase stayed voluntary in practice, and it never converted into enforcement.
That distinction matters for how a billing team spends its time. Effort spent enforcing a paused rule is effort not spent on the denials that actually cost money.
The 2024 Pause, and Why It Matters Right Now
For anyone billing CPT code 71250 today, the operative fact is this.
In the CY 2024 Physician Fee Schedule Final Rule, CMS paused the entire AUC program for reevaluation and rescinded its own implementing regulation, 42 CFR 414.94, effective January 1, 2024.
CMS stopped qualifying CDSMs entirely and removed that qualification information from its own program page. No resumption date has been announced.
The current status sits on the CMS Appropriate Use Criteria Program Status page, which no longer lists any qualified mechanisms.
A currently ranking competitor guide lists CDSM non-compliance as an error to actively prevent, without noting any of this history. That overstatement risks a practice maintaining compliance infrastructure against a requirement that carries no payment consequence right now.
Compliance rules shift, and the field’s own content doesn’t always catch up. Our denial management services stay current on which rules carry real payment consequences today, not which ones used to.
The Six-Scan Rule: Medicare’s Actual Frequency Limit for Repeat Chest CT
No identical CT chest CPT code should be ordered more than six times per calendar year, a limit that applies specifically to outpatient office, outpatient hospital, independent clinic, rural health clinic, and independent diagnostic testing facility settings.
The Rule, Stated Precisely
The limit applies to the same identical CPT code repeated for the same patient, not to chest imaging generally.
A patient who receives 71250 five times and 71260 once in the same calendar year hasn’t exceeded it, since the limit is measured per identical code.
Six is the ceiling for repeats of one exact code, not a cap on medically necessary imaging across a year.
A patient with genuine clinical need for more can still be covered, but the claim past six invites review and needs documentation that holds up.
Why This Is a Local Coverage Determination, Not a National Rule
This rule comes from a CMS Billing and Coding Article, CMS Billing and Coding Article A56580, supporting a Local Coverage Determination administered by Palmetto GBA. It covers Alabama, Georgia, Tennessee, South Carolina, Virginia, West Virginia, and North Carolina.
Practices billing CPT code 71250 outside this jurisdiction should confirm their own Medicare Administrative Contractor’s parallel LCD, since coverage articles are local by design. Other MACs may state this frequency threshold differently, or not at all.
The practical takeaway is to know your own MAC. A frequency rule that binds a practice in Georgia may read differently for a practice in Ohio, because these coverage articles are written jurisdiction by jurisdiction.
The six-scan figure is worth flagging because so little competitor content mentions it at all. A team that doesn’t know the limit exists won’t see the denial coming when a high-utilization patient crosses it.
Medical Necessity: The Shared ICD-10 List Behind 71250, 71260, and 71270
CMS establishes one combined medical necessity list covering 71250, 71260, and 71270 together, not three separate lists. It runs to thousands of individual ICD-10-CM codes under the same jurisdiction named in Section 7.
Why the Covered Diagnosis List Is So Broad
The list spans infectious disease, from tuberculosis to fungal pneumonia to sepsis, alongside malignant neoplasms and structural chest findings. That breadth reflects how genuinely wide the legitimate clinical reasons for a chest CT actually are.
A reader shouldn’t take that breadth as evidence that any diagnosis will do. It reflects clinical reality, not a loosened standard, and payers still expect the code to match the record.
Take two patients: one with suspected sepsis, one with a newly found lung mass. Completely different diagnoses, the same 71250, both legitimately on the covered list. The list is wide because the clinical need is wide.
Documenting Medical Necessity So It Survives Review
The diagnosis code on the claim has to match a genuine, specific clinical indication actually present in the record. A convenient adjacent code, chosen because it appears on the covered list, is exactly what triggers a denial on review.
A vague indication invites the denial risk this breadth might otherwise seem to eliminate. Specific beats broad every time an auditor reads the chart.
A specific symptom code can support the study when it names the real clinical concern. A vague catch-all rarely survives the same review, even when it technically appears on the covered list.
The shared list also explains why the same documentation discipline carries across all three contrast-status codes. Whichever code the contrast decision produces, the diagnosis still has to justify the study on its own, under the same CMS billing and coding article named in Section 7.
71250 vs 71271: Why Routine Diagnostic CT and Lung Cancer Screening Are Not the Same Claim
Low-dose CT lung cancer screening has its own dedicated code, CPT 71271. A routine diagnostic CT chest, billed under CPT code 71250, isn’t the correct code for a screening exam, even when neither study uses contrast.
The Coverage Pathways Are Genuinely Separate
CMS treats diagnostic imaging and screening imaging as separate coverage frameworks. The routine diagnostic pathway, covered by the frequency limit and shared ICD-10 list from Sections 7 and 8, sits under LCD L33459, Computerized Axial Tomography Thorax.
The lung cancer screening pathway sits under its own distinct framework, with eligibility tied to age range and smoking history, not a general chest symptom or finding.
Screening eligibility turns on specific criteria: an age range, a documented smoking history, and in many cases a shared decision-making visit on record. A diagnostic order rarely carries any of that, which is why the two claims can’t be swapped.
The low-dose CT screening code, 71271, sometimes shortened to the LDCT code, follows screening rules end to end. The divergence is real at the coverage level, not just administrative.
What Happens When 71250 Gets Billed for a Screening Exam
A claim that reads as a routine screening exam but gets billed under 71250 risks denial under screening exclusions. It fails diagnostic medical necessity, and it was never routed through the screening eligibility documentation the payer expects.
The fix isn’t a modifier. It’s the correct code from the start, 71271, supported by the specific age and smoking-history documentation the screening pathway requires.
This is the single ambiguity most likely to cost a screening program money. Bill the screening scan as a diagnostic study and it fails on a rule the diagnostic code was never meant to satisfy.
Prior Authorization and Radiology Benefit Managers: What Actually Gates This Claim Today
While the federal AUC program sits paused, commercial prior authorization for CT chest is very much active. For most major payers, it’s managed by a small number of Radiology Benefit Management companies rather than the payer directly.
eviCore, AIM Specialty Health, and Carelon
eviCore, AIM Specialty Health, and Carelon each process authorization requests for CT and other advanced imaging on behalf of most major commercial payers and Medicare Advantage plans. Each carries its own clinical criteria and its own submission workflow.
A practice that orders CT chest without checking which RBM the specific plan uses risks a scheduled scan that never gets approved. The plan’s card rarely tells you; the benefit details do.
What the Front End Has to Confirm Before the Scan Happens
Confirm eligibility first. Then, separately, confirm the specific RBM’s prior authorization requirement for the exact code being ordered. The two checks aren’t the same, and passing one doesn’t cover the other.
Submit with the clinical documentation and the ICD-10 code that supports the study, then record the authorization reference number and the approved services before the patient is ever scheduled.
The sequence mirrors a costly pattern. A scan performed without a confirmed authorization can leave the practice holding the full facility charge, sometimes well over a thousand dollars, with no payer on the hook.
When an RBM denies the initial request, the next step is often a peer-to-peer review between the ordering physician and the RBM’s reviewer. Building that step into the workflow keeps a medically necessary scan from stalling.
A CT chest scheduled before its authorization is confirmed is how a practice absorbs a facility cost the payer never agreed to cover.
Our eligibility verification and prior authorization services confirm both pieces, coverage and authorization, before the scan is ever booked.
Every RBM calls its process something slightly different. Our prior authorization team records the same reference number and approval scope regardless of what the payer’s portal calls it.
What CPT Code 71250 Pays in 2026
71250 is priced under the standard Medicare Physician Fee Schedule, using a work relative value unit multiplied by the annual conversion factor. The payment splits between the professional and technical components when two entities divide the work.
| Component | What it covers | 2026 figure |
|---|---|---|
| Professional (Mod 26) | The radiologist’s interpretation and report | Roughly $55 nationally, before geographic adjustment |
| Technical (Mod TC) | Equipment, technologist, and facility overhead | Varies by facility type and geography; verify via the PFS lookup tool |
| Global (no modifier) | Both components, one entity | The two components combined; varies by setting |
Professional and Technical Component Rates
The professional component for 71250 runs at roughly $55 nationally. The technical component and the combined global rate vary considerably by facility type and geography, which is why a single quoted number rarely holds across markets.
Why the Same Region Priced Differently Across the CT Family
Within any body region, the without-then-with-contrast code reimburses higher than either single-phase code alone. It requires interpreting two complete image sets rather than one, the same logic established for the chest family in Section 3.
That PC/TC split and contrast-tier pricing pattern extends across other CT and MRI regions. Learn the pattern once and it travels, rather than memorizing each code’s rate in isolation.
The same hierarchy, and the same MPPR reduction applied when a second region is imaged the same date, governs MRI billing too. Our MRI lumbar spine billing guide shows how it applies to spine imaging.
The same Tax Identification Number logic that decides whether a facility and a physician bill globally or split into components applies well outside imaging. Our echocardiogram billing guide shows the same decision in cardiac imaging.
Pull current rates for 71250 and its modifier variants live rather than quoting them from memory. The CMS Physician Fee Schedule Lookup Tool is the source for that verification.
The Denial Patterns Behind Most CPT 71250 Rejections
The Errors, Ranked
Five errors account for most 71250 denials, and each traces back to a rule already covered above.
| Denial trigger | The rule that prevents it |
|---|---|
| Wrong contrast code | Billing 71250 when the report documents contrast, or the reverse. Cross-check the report before finalizing the code. |
| Duplicate component billing | One party bills global while the other bills a component modifier. Confirm the split before either claim goes out. |
| Weak medical necessity | A diagnosis code that doesn’t match a specific indication in the record. Document the real clinical reason for the study. |
| Screening billed as diagnostic | 71250 used for a low-dose screening exam instead of 71271. Route screening through its own code and eligibility. |
| Bundling violation | Billing 71250 alongside a same-day interventional code without checking NCCI. Verify current edits first. |
Getting CPT code 71250 right on the first submission means the contrast documentation, the component split, the diagnosis code, and the correct screening-versus-diagnostic pathway all align before the claim goes out, not after the denial arrives.
Bundling violations remain one of the most common triggers here. The interaction between a chest CT and a same-day interventional code sits in the CMS NCCI Policy Manual, Radiology.
Our HCPCS versus CPT billing guide shows how NCCI checks CPT combinations against HCPCS Level II codes more broadly, the same specificity principle at work across code families.
Modifier mismatches between a professional-component claim and a technical-component claim are a recurring rejection pattern across specialties. Our clearinghouse rejections guide lays out the complete pattern.
Where Hospital-Based Billing Diverges From Independent Facility Billing
When the technical component happens inside a hospital outpatient encounter, place of service 22, that work is typically packaged into the hospital’s facility payment rather than paid as a standalone line the way an independent center’s technical component would be.
A practice expecting identical billing treatment across both settings for the same code will find the payment logic itself different, not just the amount.
Hospital-based CT billing carries payment logic that looks nothing like independent facility billing for the identical code. Our hospital revenue cycle management services are built around that packaging structure.
CPT 71250 Billing Across Ordering Specialties
A pulmonology practice’s most common CPT code 71250 error clusters around the diagnostic-versus-screening boundary from Section 9.
A hospital-employed radiology group’s most common error clusters around the technical-component packaging from Section 12. An independent imaging center’s clusters around the prior authorization sequencing from Section 10.
The underlying code and its rules stay identical across all of them. The point of failure changes by ordering context, not the code itself.
71250 is ordered across pulmonology, primary care, emergency medicine, and oncology. The specific denial risk shifts by ordering context, even though the underlying coding rules stay identical.
Picture the same chest CT ordered three ways: by a pulmonologist chasing a nodule, by an ER physician ruling out a bleed, by an oncologist staging disease. One code, three workflows, three different ways the claim tends to break.
A billing operation built around one specialty’s typical failure point misses the others entirely.
Getting this code right consistently across every ordering context requires treating the contrast documentation, the modifier split, the screening boundary, and the prior authorization sequence as one connected discipline, not four separate concerns handled by whichever department touches the claim first.
CPT Code 71250: Frequently Asked Questions
What is CPT code 71250 used for?
CPT code 71250 covers a computed tomography examination of the thorax performed without contrast material. It evaluates the lungs, mediastinum, pleura, and chest wall for infection, structural abnormality, or suspected malignancy.
What is the difference between CPT code 71250 and 71260?
71250 applies when no contrast is administered. 71260 applies when contrast is administered throughout. The radiology report, not the original order, determines which code is correct.
What modifier goes with CPT code 71250?
Modifier 26 covers the professional interpretation, Modifier TC the technical acquisition, and Modifier 59 or the more specific XS distinguishes two genuinely distinct studies on the same date. No modifier is needed when one entity bills globally.
Is CPT code 71250 used for lung cancer screening?
No. Low-dose CT lung cancer screening is billed under the dedicated code, 71271, governed by its own separate coverage pathway and eligibility criteria.
How many times can Medicare cover CPT code 71250 in a year?
CMS billing guidance limits identical CT chest code orders to no more than six times per calendar year in specified outpatient settings, under the Local Coverage Determination administered by the applicable Medicare Administrative Contractor.
Does CT chest without contrast require prior authorization?
Often, for commercial payers. Most major insurers route advanced imaging prior authorization through a Radiology Benefit Manager, such as eviCore, AIM Specialty Health, or Carelon, rather than reviewing it directly.
Is AUC or CDSM consultation still required for CPT code 71250 in 2026?
No payment penalty currently applies. CMS paused the entire Appropriate Use Criteria program and rescinded its implementing regulation effective January 1, 2024, with no resumption date announced.
Can CPT code 71250 be billed with 71260 on the same date?
Generally no, for the same imaging session. A narrow exception exists for two truly distinct, separately medically necessary studies at different times on the same date, documented and distinguished with Modifier 59 or XS.
The CPT 71250 Coding Decision Checklist
Four questions settle almost every 71250 claim.
| Ask | Then do this |
|---|---|
| Was contrast administered, and does the report confirm it? | No contrast, 71250. Contrast throughout, 71260. Non-contrast then contrast, 71270. The report governs, never the order alone. |
| Is this a screening exam or a diagnostic exam? | Screening for lung cancer, with age and smoking-history eligibility, 71271. Any other clinical indication, the contrast-status code from question one. |
| Who performed the acquisition, and who performed the interpretation? | Same entity, bill globally with no modifier. Different entities, split with Modifier 26 and Modifier TC. |
| Is there a second chest CT for this patient on this date? | Genuinely distinct and separately necessary, apply Modifier 59 or XS with documentation. If not, confirm 71270 isn’t the single correct code for one continuous study. |
Run those four in order and the code, the contrast tier, the component split, and the same-date question all fall into place.
Conclusion
CPT code 71250 billing depends on contrast documentation, correct component splitting, an accurate screening-versus-diagnostic distinction, and a prior authorization process that has real, current teeth, even though the federal AUC requirement covered here does not right now.
Getting this code right in 2026 means building a workflow around what actually carries consequences today, not around a requirement CMS paused two years ago.
Consistent, accurate CT chest billing across every ordering specialty and facility type is one part of a complete imaging revenue cycle, from prior authorization through claim submission to denial recovery.
See ClaimMax RCM’s imaging revenue cycle management services for how these pieces connect.
ClaimMax RCM manages 71250 billing across pulmonology, primary care, emergency medicine, and hospital-based radiology practices, from prior authorization and Radiology Benefit Manager coordination through accurate component billing and denial recovery.